


 Often in western films there is a scene where an arrow is yanked from the body of a fallen comrade. As dramatic as that may be it is definitely not the recommended method for removing an arrow.
Often in western films there is a scene where an arrow is yanked from the body of a fallen comrade. As dramatic as that may be it is definitely not the recommended method for removing an arrow.
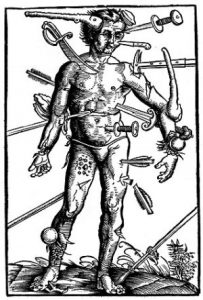
Battle wounds in the American Revolutionary War were of a wide variety, none of which were easy to treat medically. One of the worst was when the victim was struck by an arrow. While the vast majority of combatants carried muskets or rifles, bows and arrows were used, sometimes along with a musket, by Native Americans.
Medical texts during the Revolutionary War period are silent regarding the treatment for arrow wounds. The most complete and detailed account of arrow wounds and treatments is Dr. Joseph Howland Bill’s “Notes on Arrow Wounds,” which is considered the “definitive work on American arrow wounds.”[1]
Dr. Bill did not practice during the American Revolution. He served during the Civil War. However, the wounds he dealt with would have been comparable to those of the 18th century. Bill was originally from Philadelphia and attended Jefferson Medical College. After graduation he joined the U.S. Army, was commissioned 1st Lieutenant, and in 1860 was assigned to Fort Defiance, New Mexico. There he wrote his 22-page essay, “Notes on Arrow Wounds,” published in the American Journal of Medical Sciences, 1862. In less than a year Bill was transferred east. He continued to serve in the Army until his death in 1885.[2]

Bill states arrows inflict wounds “with a fatality greater than that produced by any other weapons — particularly when surgical assistance cannot be obtained.”[3] Bill understood the importance of recording his observations for the Army and future settlers as well as documenting his experiences and findings, from both living and dead arrow wound victims, for history and medicine.
Arrowheads could be made from stone, antlers, shells, hardwood, bone, or metal. The arrowheads Dr. Bill most encountered were filed metal while the shaft was usually made from a dogwood branch. For the shaft the dogwood branch was soaked, all the bark removed, and then the limb was straightened using a twisting method. This whole straightening process took about three days.[4] Feathers were also an important part of the arrow. The size and type of feather used determined the speed and rotation of the arrow. The heavier the arrowhead the larger the feathers needed to spin the arrow.[5]
Once the shaft was ready, the arrowhead was attached using tendons and sinews. This kept the head secure, until the tendon got wet. Once wet, the arrowhead would become loose and easily separate from the shaft. So, when the arrow penetrated the body the arrowhead would loosen from its contact with blood and other bodily fluids. Dr. Bill explains the worst thing a friend could do was to try to remove the arrow by pulling on the shaft, which would cause the arrowhead to be left behind forcing the doctor to search for the projectile.[6]
In some situations the arrow proved more destructive to the victim and more difficult to treat for the doctor than a gunshot wound.[7] The problems came from the nature of arrow warfare and the shape and texture of the projectile. Dr. Bill estimates an “expert bowman can easily discharge six arrows per minute.”[8] In one of Dr. Bill’s cases three soldiers suffered a total of 42 arrow wounds between them. Although this number of wounds was extreme, Bill states he rarely saw someone with a single arrow wound.[9]

Further complicating the multiple wounds was that each arrowhead had to be removed. Unlike a gunshot wound, the arrowhead must be located and extracted. Arrowheads were rough and sharp. No tissue around the arrowhead could heal and in the body’s attempt to rid itself of the foreign object infection would rage forming an abscess. Every time the victim moved the arrowhead’s rough edges would inflame and aggravate the injury and eventually lead to a fatal infection or amputation.[10] In contrast a 18th century bullet did not have the sharp edges and could become encysted in tissue or encased in bone and safely remain in the body. The importance of removal is clear in Dr. Bill’s instructions: “We might as well cut the patient’s limb up until we do find the arrow-head.”[11]
Now the gravity of a friend’s attempt to pull the arrow from a wounded comrade becomes apparent. If the shaft was left in place, Dr. Bill’s treatment was to make an incision to enlarge the entry wound and slide a finger down the shaft to feel the depth of the wound and determine if the arrowhead is lodged in bone.[12] Without the shaft in place the doctor was forced to search for the arrow by making a larger incision, probing through tissue, causing more trauma, and taking more time. It was much easier for the doctor and patient if the shaft was left intact until a doctor could remove the head and shaft as one piece. Further, there was always the danger that the arrowhead could not be found leaving the “angular and jagged head… buried in bone to kill – for so it surely will.”[13] If, however, the arrowhead is removed properly, the wound was likely to heal naturally.[14]
If lodged in bone, the doctor could expect to use great force to remove the head. Special instruments were usually employed for this procedure. For instance, a wire loop was often used to grasp the arrowhead, but Dr. Bill frequently reported using strong dental tooth-forceps.[15] The doctor would guide the forceps down his finger and onto the arrowhead.[16] Once the forceps grasped the arrowhead the finger was withdrawn and traction could be applied. Sometimes, however, the arrowhead would be lodged so deeply in bone the forceps would bend from the force of the traction used.[17]
One method to determine if the arrowhead was lodged in bone was by “twirling the shaft,” if the shaft moved the arrowhead was declared not to be lodged in bone.[18] The force needed to remove an arrowhead embedded in bone was surprising. In one particular case Private Bishop was hit in the upper arm near the shoulder. Dr. Bill describes his effort; “…and bracing my knees against the patient’s thorax, I applied all the traction I could muster. Suddenly the arrow-head flew out of its seat, and I would have fallen on the floor, had not the steward caught me.”[19] In 1876 Dr. Bill presented his own design of forceps specifically for removing arrowheads.[20]
Much of the victims’ chance of survival depended on where they were injured and how deep the wound. A number of injuries to the arms were reported, probably because soldiers would attempt to shield themselves with their arms and hands.[21] If the arrow went through a limb it would usually heal normally. The entrance wound appeared as a “very small and narrow slit“ surrounded by a reddish bruise while the exit wound would be larger but without the bruise.[22] For the treatment of this kind of wound Bill would apply “cold or evaporating lotions” and order the patient to allow the injured arm or leg to rest. Meanwhile Bill would watch for any sign of infection which he would treat with “bandages, compresses, and an early evacuation” of any drainage if necessary. Barring any infections, however, the injury would generally heal in a week.[23]
Complications could occur, however. For instance, even though doctors knew how to treat a severed artery, medical help often could not be obtained in time to stop the victim from bleeding to death. Other complications included fractures, broken bones, and severed nerves, but if the arrowhead was removed these injuries were not usually fatal.[24] One particular example of a complication and Bill’s skill is that of Private Martin of the 3rd Infantry. Martin suffered an arrow wound to his right leg; while the arrow did pass through, Martin was left with “agonizing pain” in his toes and foot. The arrow had injured a major nerve, which Dr. Bill divided to stop the pain.[25]
One particular complication of limb wounds involved muscle contractions. If the arrowhead “scrapes the bone near the edge” it could cause a muscle contraction so forceful the metal arrowhead tip was bent to resemble a “fish-hook.”[26] Apparently this complication was common enough for Bill to write “that the digital examination of arrow wounds should always be practised” because if the arrow head is bent upward pulling on it would only injure the victim more.[27] Two precautions should be taken. First, the doctor should push down on the arrowhead to dislodge the hook and then the doctor’s finger should remain on the curved point of the arrowhead during the removal “in order to prevent the entangling” of the hook in any tissue.[28] Bill treated two men who suffered this complication. In the first injury the arrowhead had wrapped around the ulna in the forearm, and the second, around the fibula in the lower leg.[29]
Some of Bill’s most interesting cases involved the head. Bill reports on a total of five head wounds. In three of the cases the brain was wounded and two men died and in the two cases where the brain was not injured both men lived.[30] Unless the arrow was fired straight at the head from a short distance it usually did not penetrate the skull. According to Bill the danger of a headshot came mainly from compression of the outer table of the skull since few arrows reached the brain itself.[31] The result of cerebral compression can include unconsciousness, slowed respirations, high blood pressure, fever, and rapid pulse.[32] Thus, the doctor would have to not only remove the arrowhead but also trephine the skull to release the pressure.[33] Usually fatal were hits to the “orbit” or eye socket but Bill never treated this particular wound himself.[34]
A post guide named Miguel was hit on the left side of his skull by an arrow. By the time Miguel reached Bill someone had removed the shaft and Miguel was suffering from the symptoms of compression sickness. Bill prepared to trephine the skull after he removed the arrowhead. However, once the arrowhead was dislodged “symptoms of compression at once vanished, the man turned over and sneezed, and rose up on his feet.”[35] Later Miguel had to be treated for a headache but otherwise recovered fully.[36]
A great deal of Dr. Bill’s essay describes wounds of the trunk. The chest and abdomen represent the largest part of the human body and house the majority of the major organs. The bowmen knew that a hit to the trunk was likely to be fatal and is where they aimed. Thus, the trunk received more injuries than other areas of the body.[37] Moreover, particular care had to be allotted for all trunk injuries until the location and depth of the wound could be ascertained because any arrowhead could be potentially lodged in the spine, which was usually fatal.[38] Bill would use his knowledge of anatomy and arrow wounds to ascertain if an arrowhead was more likely to be lodged in a rib or vertebrae from the length of the exposed shaft.[39]
An arrow wound to the lung, explains Bill, is much more dangerous than a gunshot wound for three reasons: amount of blood loss, infection, and emphysema. For example, arrow wounds cause more bleeding than gunshot wounds because an arrow “makes clean slits and punctures” while a “ball tears and bruises.” Bill also explains arrows tend to lodge themselves in the lung “whilst a ball generally passes” causing empysema, an infection in the body cavity.[40] Bill states the “third danger peculiar to arrow wounds of lung is the supervention of emphysema” about twelve hours after the injury occurred.[41] Emphysema is a condition where the air spaces in the lungs are distended causing difficulty in breathing.[42] However, Bill goes on to say that the onset of emphysema is more of a nuisance than danger.[43]
Of the fifteen men Bill saw with chest wounds, six had injured lungs and four of them died. Of the nine men without injuries to the lungs all survived.[44] The wide range of chest injuries Bill encountered demonstrates the nature of complications possible. From the five detailed cases that included chest wounds, chest wounds were usually accompanied by infections, such as the case of Salvador Martinez. An arrow entered Martinez‘s chest “between the fifth and sixth ribs on the right side, and passed out between the seventh and eighth on the left.”[45] When Martinez saw Dr. Bill he was having difficulty breathing and in great pain. Bill treated Martinez aggressively for sixteen days but was unable to save him. Upon a postmortem examination Bill found the right lung “solidified and engorged with pus” and the left lung also full of infectious matter.[46]
Abdominal wounds also proved to be exceedingly dangerous because unlike the lungs the abdomen is not protected by the rib cage.[47] Of Bill’s twenty-one abdominal cases all but one was fatal.[48] As Bill states, “Arrow wounds of the abdomen are generally fatal. An arrow can scarcely pass through the abdomen and fail to open a vessel or wound an intestine.”[49] If the abdominal wall is breached the main threat is from a hemorrhage or an infection resulting from a punctured intestine. Bill recommends enlarging the wound in order to examine the abdominal cavity. If the intestines are lacerated, gold wire was used to suture the injury.[50] Again, the arrowhead must be removed if the patient was to have a chance at recovery.
Overall Bill reports he “observed” eighty arrow wounds, the majority to the trunk, thirty-six in all. Of these thirty-six men injured twenty-two died. The extremities are next with a total of 35 wounds.
Bill’s observations from treating the wounded as well as his empirical postmortem research provided the medical community then and the history community today with the only documentation for the nature and treatment of arrow wounds.
The author wishes to thank Lisa A. Ennis for her assistance with the research of this article.
[3] Bill, Joseph Howland, “Notes on Arrow Wounds,” American Journal of Medical Sciences, 154, 1892, p. 366.
[5] Stockel, H. Henriette, The Lightning Stick: Arrows, Wounds, and Indian Legends, Reno, University of Nevada Press, 1995, 47-48.



14 Comments
What a read! You never disappoint, well done on this one Hugh. I was a little squeamish at times as I read just imagining the excruciating pain these men went through not only being shot by the arrow but then having it removed in a time when anesthesia as we know it did not exist!
It’s funny but it always seems so noble in the movies when someone gets shot by an arrow in the abdomen and pulls it out only to continue fighting until the battle is won through their bravery and leadership.
I suppose it wouldn’t make a good movie if the hero was shot by an arrow only to fall off his horse to certain death.
Michael, Glad you enjoyed the article. When I came across this topic I realized that I knew absolutely nothing about treating arrow wounds….other than Hollywood. I was very pleased to be able to find Dr. Bill’s detailed report. Thanks for your comments.
I’ve been researching the 18th-century for nearly 40 years and don’t remember a single comment about treating arrow wounds. I’ll bet there aren’t a half-dozen of all the learned folks studying the period who know anything about this topic. Until now, that is. Many thanks, Hugh.
Mike – Thank you very much for that wonderful compliment. I try to find topics that are more obscure. No sense in repeating what everyone already knows. So many outstanding researchers have covered so much ground that finding “untilled soil” is a problem. However, when some out-of-the-way topic is found research can be aimed at that specific point…and, with luck sometimes something useful can come of it. Thanks, again.
Hugh, the Army’s Surgeon General’s department released a study in 1871 of wounds between 1865-1871 which it deemed instructive. The study is at archive.org and is entitled “A Report of Surgical Cases Treated in the Army of the United States from 1865-1871”. If you download it, on the p. 149 of the PDF reader there is a section on arrow wounds with an brief introduction to historical medical practitioners who wrote about arrow wounds. The archive.org URL is:
https://archive.org/details/areportsurgical00otisgoog
Incidentally, excellent article about Dr. Bill.
Billy,
Glad you liked the article and thank you for the information on this 1871 source. I had not been aware of it. FWIW I find archive.org is a wonderful resource.
Thanks again.
This is a very interesting read. I am in the process of writing a Fantasy trilogy, and the bow and arrow is a weapon used in abundance. This article is very informative and will help tremendously in my writing of injuries sustained by this weapon. Thank you for your information.
Well, the ”emphysema” that Dr Bill describes is actually a pneumothorax that causes shortness of breath and if it is was tension pneumothorax, then it would be life threatening. A big problem of this puncture wounds was infections, as antibiotics that days did not exist. So, if the patient survived from the bleeding, the he may die from infection, including tetanus. But even for bleeding, except surgical hemostasis, fluid rescue infusions (such as saline) also did not exist. In conclusion, an arrow puncture wound would be a great challenge for the doctor, however many of the victims suprizingly survived, perhaps because during the war it was difficult to targen with effectively the victim, especially if the indian was up on a horse. Thus, many injuries were superficial.
Excellent! I need to learn how serious a spear wound might have been, but survival. What would have been the first steps taken by rangers? Would one have probed the wound to promote bleeding, applied sugar or honey. This ranger survived a Comanche spear and was transported to San Antonio a few days later In a wagon where he eventually recovered.
Fascinating article. I am a historian of Chinese medicine researching the treatment of arrow wounds in China from the 6th to 19th century. Arrowheads stuck in bone were a standard problem for them as well. They used “numbing drugs” to ease the pain of removing them (with pincers). Good to have these comparative perspectives from American medicine!
How fascinating! Similar to another commenter, I am also a simple writer perusing historical articles on weaponry and injuries. This was extremely helpful!
Great article – and you have an excellent grasp on the medical issues! The infection which could occur with an arrow wound would arise from bacteria carried into the tissues with the arrow itself, or after the wounding via entry of environmental bacteria through the cutaneous defect or from the surgeon’s exploring hands or instruments, unless sterilized (which they weren’t, until Lister) . (President James Garfield died from just such iatrogenic infection). As another commentator mentioned, tetanus would be a real threat.
We have one detailed account of the removal of an arrow head and the treatment of the wound from 1403. While fighting in the Battle of Shrewsbury on July 21st 1403, the 16 year old Prince Henry (later King Henry V) was hit in the right side of his face by an arrow. He refused to leave the battlefield and fought on after having had the shaft of the arrow removed. Once the royal army had defeated the Percy rebels, Prince Henry allowed his injury to be examined and it was clear that the arrow head was lodged about six inches into his cheek.
The London surgeon John Bradmore was summoned to see if he could remove the arrow head. He later left a detailed account of his treatment of the prince:
“First, I made small probes from the pith of an elder, well dried and well stitched in purified linen [made to] the length of the wound. These probes were infused with rose honey. And after that, I made larger and longer probes, and so I continued to always enlarge these probes until I had the width and depth of the wound as I wished it. And after the wound was as enlarged and deep enough so that, by my reckoning, the probes reached the bottom of the wound, I prepared anew some little tongs, small and hollow, and with the width of an arrow. A screw ran through the middle of the tongs, whose ends were well rounded both on the inside and outside, and even the end of the screw, which was entered into the middle, was well rounded overall in the way of a screw, so that it should grip better and more strongly.”
His approach was to slowly widen the wound using wooden probes wrapped in clean linen and then rolled in honey – a natural antisecptic. Once he was able to probe to the base of the wound, he used his specially constructed tongs to penetrate to the end of the arrow head and remove it. All this was conducted without anaesthetic and would have been excruciatingly painful for Henry, though leaving the arrow head in would almost certainly have resulted in an even more painful death from infection.
Once the arrow head was removed, Bradmore washed the wound with white wine and then cleaned it with another linen-wrapped probe soaked in honey, before binding it with more clean linen. He repeated this process every day for 20 days, though each time he made the probe he used slightly smaller, allowing the wound to close up as it healed.
By the end of the process the wound had fully healed and the prince survived, though he was left with a large scar on his cheek.